Anterior Cervical Decompression & Fusion
 Anterior Cervical Decompression & Fusion (ACDF) is a procedure that involves approaching the neck through the front of the spine.
Anterior Cervical Decompression & Fusion (ACDF) is a procedure that involves approaching the neck through the front of the spine.
The aim of the operation may be to decompress the spinal cord (causing myelopathy) or a nerve root (causing arm pain).
It may also be performed to correct a deformity of the neck or in cases of neck instability.
The cervical spine is approached through the front, with the incision usually being in one of the skin creases.
In most cases, this is through the right hand side (for a right-handed surgeon).
A plane is developed between the main blood vessels passing through the neck and the windpipe (trachea) and gullet (oesophagus).
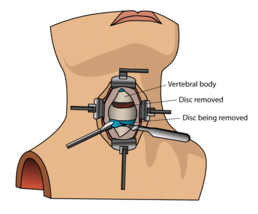
Using a microscope, the disc is removed and the spinal cord as well as the roots are decompressed.
The space left is replaced by a cage (usually made of a special plastic called PEEK) and secured with a plate.
In some cases an implant integrating both principles may be used.
Cervical Laminectomy
 Cervical Laminectomy is performed to decompress the spinal cord in cases of myelopathy.
Cervical Laminectomy is performed to decompress the spinal cord in cases of myelopathy.
The patient is usually placed prone (face down) with the head supported by a clamp.
An incision is made on the back of the neck and the muscles moved to either side to expose the bony elements.
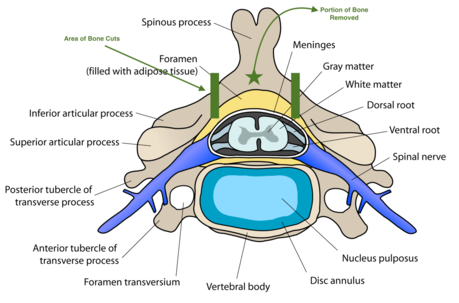
The lamina and spinous process are then removed of the affected level, thereby decompressing the spinal cord.
In some cases where there is pre-existing instability, this may be supplemented by fixation with screws and rods at the same time.
Cervical Disc Replacement
In select cases, motion preserving technology (disc replacement) may be used.
Despite its theoretical advantages, long term results demonstrate that they are at least as good as ACDF procedures.
However, patient selection is essential.
The main indication is young patients with no neck deformity, instability or myelopathy.
The approach and procedure are essentially the same as an ACDF, however more x-rays are required as positioning is essential.
Deformity Correction
Deformity correction surgery covers a vast array of spinal deformities.
These include idiopathic scoliosis and kyphosis in younger patients to adult degenerative deformities in the older age group.
The exact procedure and technique is patient-specific but may include screw fixation at multiple levels, bony cuts to correct the spine (osteotomy) as well as releasing the spine completely and realigning.
Occasionally the procedure involves going through the chest or abdomen as well as through the back.
Deformity correction is usually performed by two spine consultants to reduce the risks.
Techniques such as intra-operative cell salvage and spinal cord monitoring may also be used.
Microdiscectomy & Microdecompression
Microdiscectomy & Microdecompression of the Lumbar spine are one of the commonest spine procedures performed.
These defer from a lumbar laminectomy (which removes all of the bone from the back of the spine - as in cervical laminectomy) as the aim is to minimise any disruption to the stability of the spine.
The procedure is performed with the patient in the prone position (face down) on a special operating table.
After x-rays are performed to mark the level, a midline skin incision is made and the muscles on the side of surgery are cleared to expose the spine.
Before proceeding, another x-ray is taken to check the correct level.
 At this point a spinal microscope is bought into the operating area.
At this point a spinal microscope is bought into the operating area.
This offers better visualisation of the neural elements.
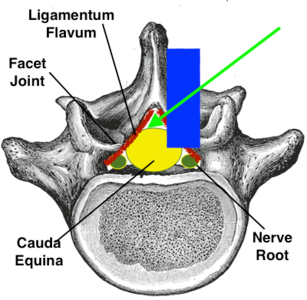
In a microdecompression, parts of the bone is cleared (laminotomy) and a portion of the facet joint may be removed (medial facetectomy) to create for the nerves (blue area on diagram).
This is followed by removal of the yellow thickened ligament (ligament flavum) which is frequently a cause of the compression.
Micro decompression may then be repeated on the other side of the spine, thereby leaving intact the important ligaments in the middle of the spine.
Alternatively, an over the top decompression may be performed (direction of green arrow on diagram).
This is technically more challenging, but offers the advantage of leaving the muscles, soft tissues and joints on the other side of the spine intact.
This reduces risks of late instability as well as quicker recovery.
Microdiscectomy uses the same approach and technique.
However, the nerves are moved to one side to expose the disc.
Any loose fragments of disc are removed (sequestrectomy).
The disc space may be exposed (annulotomy) and any free fragments are removed.
Spinal Fusion
Spinal fusion (such as a PLIF) is a surgical technique to stabilise the vertebra and the disc between the vertebra.
Lumbar fusion surgery is designed to create solid bone between the adjoining vertebra, eliminating any movement between the bones.
The operation aim is to do the following:
-
Restore the normal height of the disc
-
Free any trapped nerves
-
Remove the pain source – the degenerate and inflamed disc
-
Correct any deformity – like a forward or sideways slip of a vertebra
-
Fuse the disc- by packing bone into the disc
-
Restore normal load transmission across the disc
 The bone graft does not form a fusion at the time of the surgery.
The bone graft does not form a fusion at the time of the surgery.
Instead, the bone graft provides the foundation and environment to allow the body to grow new bone and fuse a section of the spine together.
At the time of the fusion surgery, instrumentation (e.g. screws and rods) is typically used to provide stability for that section of the spine for the first few months after surgery.
Over the long term, a solid fusion of bone that has healed together provides stability.
Spinal Injections
Lumbar Spine Nerve Root Block Injections
This is due to the pain in one or both of your legs which is thought to be caused by irritation or inflammation of the nerves in the bottom part of your spine.
The injection can reduce inflammation and provide pain relief, and also help to clarify where your leg pain is coming from.
About the Procedure
The injection consists of local anaesthetic and steroid being placed around a specific nerve as it exits the spine.
It is performed as a day-case procedure and may be performed with you awake in the operating theatre.
The needle is placed under x‐ray guidance, and its position confirmed by injecting a small amount of dye that shows up on the x‐ray.
Please inform a member of staff if you think you could be pregnant as x-rays could harm the foetus.
You will be allowed home soon after the procedure but will need someone to take you.